In 2007, under-engineering, inefficient regulation, ever increasing dead loads combined with inept inspections led to the deadliest structural failure in Minnesota’s history.

On the first day in August 2007, contractors in charge of the remedial works on the I-35 highway bridge in Minneapolis, Minnesota were preparing for a concrete pour on the southbound lanes of the bridge. Several concrete pours have been completed since the start of the remedial operation in July, with this very one under preparation seemingly being the eight, and scheduled for 7pm the same day.
One of the contractor preparation strategy involved stockpiling the concrete materials (gravel and sand) on the southbound lanes. Aside the fact that having these materials close to the place of concrete placement would ease the pouring operation, Minneapolis Department of Transport’s MnDOT specification only provided an hour window between initial concrete mixing and final screeding, thus it wasn’t to be an unusual operation2. By afternoon, about 264t of load from construction materials, construction vehicles, equipment’s and personnel were already in place for the concrete pour.
Well, as we now know, that pour never took place because a few minutes past 6pm that day, a section of the bridge main truss collapsed, falling 33m into the river below (Figure 1). There were 13 fatalities and more than 100 casualties. In this article, we’ll be exploring the I-35 Bridge and the circumstances in which it collapsed, particularly the role played by implicit assumptions in covering up the design flaw as it went unnoticed for 40years, amidst several design reviews and remedial works.
The I-35W Bridge
The I-35W Bridge also known as Bridge 9340 was an eight lane, steel truss arch bridge, designed to carry interstate traffic across the Mississippi River. It was 580m long, carried 8 lanes of traffic (four northbound and four southbound), and comprised of 14 spans (Figure 2). The three main spans are made of truss construction while all but two of the approach spans used a steel multi-girder construction. The two exceptions were made of concrete slab construction.

The I-35W bridge was designed by consulting firm; Sverdrup & Parcel and Associates. The bridge opened to operation in 1967 and shortly after became the third busiest bridges in the state of Minnesota, carrying over 140,000 vehicles a day.
The I-35 Bridge had been designed prior to the theory of metal fatigue being understood by designers. In the late 1970s when a better understanding of this theory became established throughout the engineering industry, deck truss bridges such as the I-35w would be recognized as non-load path redundant or fracture critical. In literal sense, if certain main truss members failed, the bridge would collapse.
Prior to this failure, three major remedial works have been carried out on this bridge each of which increased the dead loads on the bridge. The first was in 1977, when a wearing course was applied on the bridge. Ironically, this was to be a solution to battle ongoing effects of road chemicals that have being corroding rebars on the top deck of bridges in similar climates. This operation involved reeling of 6mm of bridge deck and replacing it with 50mm of low slump concrete. This brought the total bridge deck thickness to over 8 inches and added more than 1300t of static load.
The second remedial operation occurred 21years later in 1998. This time, the renovation/modification involved replacing the medium barrier, upgrading the concrete traffic railings, improve drainage, repair slabs, retrofit cross girders and the installation of an anti-icing system. In all the 1998 remedial works added another 450t of dead loads. The third remedial operation was underway when this collapse occurred. It involved replacement of the entire wearing course again, during which stockpiling of materials on the bridge occurred.
Investigation into Cause of Failure
Following the collapse, the National Transportation Safety Board (NTSB) immediately began a comprehensive investigation that would go on to take eighteen months. The exercise would come to a close with the NTSB concluding that undersized gusset plates due to a design error in combination with recent increases in dead and live loads as the cause of the failure. How did the NTSB reach this conclusion? This would be expatiated in the subsequent sections.
Stockpiling Operation
As said, one of the discoveries of the NTSB was, recent increases in dead and live loads contributed to the failure, one of these loads was from stockpiled materials. The NTSB would discover that load from the stockpile alone was up to four times the design live load of the bridge. This estimate was based on eyewitness accounts, post incident vehicle positions and more interestingly from a photograph taken by a passenger on a commercial airliner, approximately 2 hours to the incident (Figure 3)2.
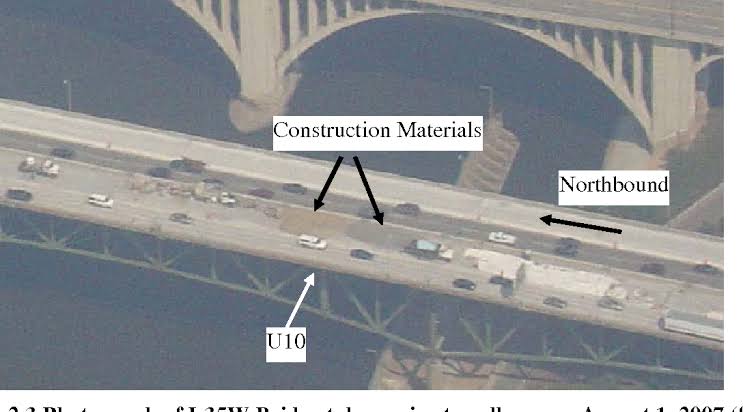
Why was the contractor permitted to stockpile such magnitude of material on the bridge and who gave the approval?
It is customary for Minneapolis Department of Transport to provide onsite inspectors whenever a remedial work of this nature is being carried out. Apparently, the onsite inspectors provided for this project were not trained. When the NTSB raised questions regarding stockpiling, the Minneapolis Department answered by saying, issues around stockpiling should’ve being directed to the bridge project engineer. However, such policy requiring contractors to obtain such permission didn’t exist at the time. During the first concrete pour in the course of the project, the contractor foreman requested if materials could be staged on the span, MnDOT onsite inspector raising no objection or concern, the foreman then interpreted this literarily as permission granted. Hence during preparations again on Aug 1st, the contractor commenced stockpiling again without permission from any Minneapolis Department engineer.
Subsequently, the NTSB then set out to even discover if Minneapolis Department would’ve granted permission, should such a request from the contractor had been received. The Minneapolis Department argued that with the load from the stockpiling being four times the design live load, they were most unlikely to have granted such a request without undertaking an analysis to verify structural integrity. The NTSB requested that Minneapolis Department undertake this analysis and interestingly Minneapolis Department would report that the load rating indicated that the stockpiling was satisfactory. Hence, the conclusion is that, should the contractor had requested for permission, Minneapolis Department relying solely on this analysis, would’ve granted permission to the contractor. If the load rating was indeed okay to support the stockpile, then what could’ve possibly caused this collapse?
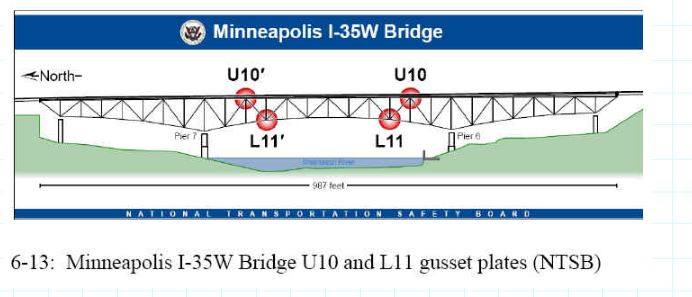
The NTSB would discover that Minneapolis Department had conspicuously ignored load ratings of the bridge gusset plates. The investigation revealed that although the load rating for main bridge members was satisfactory, a sizable number of gusset plates had been undersized due to a design error. Having determined the actual capacities of the gusset plate on the collapsed span of the bridge, it was evidently clear that the increases to the bridge dead load coupled with the weight of materials stockpiled on the bridge on August 1st was sufficient to overstress the structure. Consequently, the NTSB would report that, had the gusset plate been designed correctly the loads from the stockpile would not have being sufficient to cause the collapse.
So, how did this design flaw go unnoticed for 40years amidst, internal design review, design reviews by both the MnDOT and the FHWA? And also, despite the bridge being subjected to two load ratings and the bridge being inspected perhaps, more regularly than required by best practice?
The Design Flaw
The NTSB would request for the original design calculation be made available by the design firm. The calculation sheets for the affected gusset plate could not be recovered. Partly due to the original design firm, Sverdrup & Parcel being absorbed by another design firm, Jacobs Engineering Group. However, a former Sverdrup & Parcel employee for whatever reasons, personally retained some records of the gusset plates calculations. Hence, NTSB was able to lay its hands on a design document that showed indeed how the design firm might’ve arrived at its design conclusions. Apparently, the critical gusset plates thickness (Figure 4) was estimated solely based on forces expected to pass into the connection through the chords. Considering these forces alone, would appear that the gusset plates have being sized correctly. However, their correct design would’ve been to include the effect of shearing forces from the truss verticals and diagonals2. This would’ve led to an increase in the gusset plate thickness.
Surprisingly, the NTSB also uncovered that while other gusset plates were thickened between the preliminary and final design stage, the final thickness of the critical gusset plates were not increased remaining as shown in the preliminary calculations1. Thus, the NTSB would also conclude that this wasn’t a case of the design firm not knowing how to correctly design gusset plates as indicated by its correct design of other gusset plates. It simply did not perform all the necessary calculations for the main truss gusset plates of the I-35 bridge resulting in the plates having insufficient capacity.
Inadequate Review
Shall we agree temporarily that this was a case of a design oversight; a situation whereby the design engineer had mistakenly omitted the critical loading condition in the design of these gusset plates. However, what happened to the internal review engineer, what happened to MnDOT and what happened with FHWA?
Next, the NTSB turned to investigate the design firm review procedures in-order to discover if they indeed had in place procedures that provides for appropriate review, including those that would had allowed for the review of gusset plates calculations. It was discovered that the design firm did not have an explicit procedure for ensuring all necessary calculations were actually performed. And thus, the conclusion was made that such a review process was inadequate.
In the case of MnDOT and the FHWA, it was found that these authorities had provisions and procedures for checking calculations, these procedures however, did not extend to checking gusset plates. Hence not only did this authority failed to discover this design error, their review provisions weren’t even equipped to do so.
Ineffective Inspections
From 1993 up until collapse, the I-35W bridge was inspected annually by MnDOT1. This was in fact more than the requirement of the National Bridge Inspection Standard. In the years leading to the collapse, several reports cited problems with the bridge structure, in fact it was given a “structurally deficient” rating twice. However, at no point during these inspections would this error ever had been discovered because the focus was on verifying condition and not to determine design errors.
Except that, there were visual evidences in about 8 of the truss gussets plates which the NTSB would later describe as characteristic of the inadequate capacity of the gusset plates. Photographs taken by contractors engaged with undertaking the strain gauging of the bridge visibly showed bowing in some of the critical gusset plates2. Perhaps, the overarching theme regarding these ineffective inspections can be summed up in the attitude of one of MnDoT’s district engineer, who specialized in fracture critical bridge inspections, who was aware of bowing in the bridge gussets. When interviewed by investigators, would informed them that he believed this bowing to have occurred during construction of the bridge1. And that gusset plates were more designed conservatively, even having a safety factor of 2 to 31. One can then conclude that, as a result, the bowings were never reported in any investigation report and the NTSB found no evidence of any analysis carried out to find out the reasons for these distortions and to what extents it had affected the load carrying capacity of the gusset plates.
Inept Load Ratings
Prior to the third remedial work that led to the failure of this bridge, recall two major remedial work had been undertaken, in 1977 and 1998. Each of these instances, presented an opportunity to determine the load rating for the bridge. However, neither of them considered the gusset plates. The NTSB reported that, had AASHTO included gusset plates in load ratings, they would’ve been at least two opportunities to unravel this design error.
Very interestingly, the NTSB would as well find that the reason for this neglect at every level was due to the belief amongst bridge designers, that gusset plates were more conservatively sized relative to the members they connect. Hence, once the capacities of the truss members were found to have been satisfactory, the gusset plates were also assumed to have sufficient capacity.
Lessons from Failure
We see time and again the role played by human factors in catastrophic failures particularly, ‘implicit assumptions’. One is tempted to just say the cause of this failure was as a result of undersized gusset plate, but the design of gusset plates was well understood. The question is, why would this design flaw go unnoticed for 40years, despite the original design being subjected to multiple reviews and load ratings?
Primarily because the reviews didn’t consider the load rating of the gusset plates. And why didn’t the review consider the load rating of the gusset plates? There is no better reason for this omission than the implicit assumption held to the heart by most bridge designers that gusset plates were more conservatively designed than the members they connect.
The failure of I-35 bridge is a reminder of the problem of implicit assumptions and why be must strive to always combat the threat it poses to structural engineering.
See: Implicit Assumptions & Expertise in Engineering

Sources & Citations
- National Transport Safety Board (2008) Highway Accident Report, Collapse of I-35W Highway Bridge, Minneapolis, Minnesota, August 1, 2007 [Online] Available at: www.dot.state.mn.us/i35wbridge/ntsb/fi nalreport.pdf (Accessed: June 2022)
- Brady S (2013) The I-35W Highway Bridge collapse: les, The Structural Engineer, Oct, 2013 available at www.IstructE.com (Accessed: June 2022)
Thank You!